


1Department of Dermatology and 2Department of Pathology, Shiga University of Medical Science, Setatsukinowa, Otsu, Shiga 520-2192, and 3Department of Dermatology, Osaka City University Graduate School of Medicine, Osaka, Japan. E-mail: kokubu@belle.shiga-med.ac.jp
Accepted Jun 4, 2020; Epub ahead of print Jun 9, 2020
Acta Derm Venereol 2020; 100: adv00204
Paraneoplastic pemphigus (PNP) is caused by humoral and cell-mediated autoimmune reactions (1). On the other hand, Stevens Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are related to drug-specific T-cell-mediated cytotoxicity. We present here a rare case of PNP mimicking TEN, which was treated with plasma exchange (PE) and showed that a cell-mediated immunity has a significant role in the pathogenesis of TEN/SJS-like PNP.
A 67-year-old Japanese woman without medication history noticed erythema on her trunk and hands and lip erosions in 2017. The erythema spread to her whole body within one month. She presented with fever of approximately 38°C, eye discharge, eye pseudo-membranes, and confluent target-like and maculopapular erythema (Fig. 1a). Laboratory investigation revealed elevated levels of soluble interleukin (IL)-2 receptor (1,830 U/ml). Blood cell counts and serum lactate dehydrogenase were within normal limits. No active infections, including Mycoplasma pneumonia and herpes simplex virus, were observed. Antibody against human T-cell leukaemia virus type 1 was negative. Histopathological examination on the upper arm showed necrotic keratinocytes in the epidermis and vacuolar degeneration of the basement membrane zone with mononuclear cell infiltration (Fig. 1b). Computed tomography scan showed a soft shadow behind the pancreas and a slight enlargement of lymph nodes, with a size of up to 14 mm, in the neck, axilla, lesser curvature of stomach, and mesocolon. We regarded this as reactive lymphadenopathy due to cutaneous inflammation. We initially diagnosed her with SJS. Various treatments were given, including oral prednisolone (1 mg/kg), and intravenous immunoglobulin (IVIG; 400 mg/kg for 5 days). However, further erosions appeared (Fig. 1c), and a second skin biopsy showed epidermal necrosis (Fig. 1d). Moreover, erosions developed on more than 30% of the patient’s entire body surface area (Fig. 1e). Therefore, we diagnosed TEN.
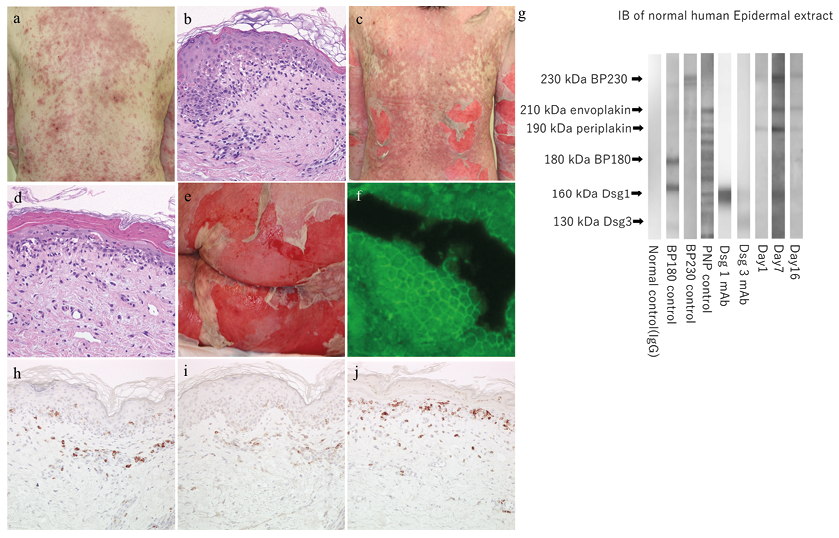
Fig. 1. (a) Clinical presentation at first visit. (b) Histopathological examination on the upper arm at first (haematoxylin-eosin (H&E) ×40). (c) After 2 days, erosions appeared. (d) The second skin biopsy on the abdomen (H&E×40). (e) Erosions appeared on more than 30% of the body surface area. (f) Indirect immunofluorescence (IIF) revealed IgG deposition. (g) Immunoblot analysis (lane 7, on admission; lane 8, before plasma exchange (PE); lane 9, after PE). Serum on admission reacted with PP (lane 7). Before PE, serum reacted with PP and envoplakin (EP) (lane 8). After PE, serum remained to react with periplakin (PP) and EP (lane 9). Sera of control, bullous pemphigoid (BP) 180, BP230, PNP, and desmoglein (Dsg)1 and Dsg3 monoclonal antibodies are shown in lanes 1 to 6, respectively. Molecular weights are indicated on the left. (h, i) Immunohistochemical staining of the first biopsy revealed more CD8+ lymphocytes than CD4+ cells infiltrated into epidermis (amino-9-ethylcarbazole (AEC), CD8 (h), CD4 (i) staining ×200). (j) Immunohistochemical staining revealed CD8+ lymphocytes infiltration did not decrease after PE (AEC, CD8 staining ×200).
The patient was treated with PE 8 times from 7 days after hospitalization; however, the erosions spread further, and she died due to septic shock. Autopsy revealed follicular lymphoma in the lymph nodes. Direct immunofluorescence (DIF) and indirect immunofluorescence (IIF) assays revealed linear IgG deposition on the basement membrane zone. IIF using rat bladder epithelial cells revealed IgG deposition (Fig. 1f). The index values of anti-desmoglein 1 (Dsg1) and 3 (Dsg3) antibodies were 49.3 and 81.2, respectively, by enzyme-linked immunosorbent assay (ELISA). Immunoblot (IB) analysis was performed for 3 serum samples collected at different time courses using normal human epidermal extract, which detected 210-kDa envoplakin (EP) and 190-kDa periplakin (PP) (Fig. 1g). Therefore, we finally diagnosed the patient with TEN/SJS-like PNP associated with subclinical follicular lymphoma. Dsg1 and Dsg3 were negative by IB analysis. Autoantibody against 210-kDa EP appeared, and the band of 190-kDa PP became clearer after IVIG. ELISA revealed that the antibody titre indexes of Dsg1 and Dsg3 remained similar on day 14 and decreased on day 16 (Fig. S1). However, the skin erosions spread day by day. We concluded that PE could not improve TEN/SJS-like PNP.
To our knowledge, there have been only 9 case reports of TEN/SJS-like PNP published in English, including the case reported here (2–8), although a systematic review showed TEN-like PNP patients were 11.8% of the total cases of PNP and have a poor prognosis (9). Eight cases had anti-Dsg 3 antibody or autoantibody against EP. In order to distinguish between PNP and TEN/SJS-like PNP, it is important to search for haematological malignancy, and to perform ELISA and IB analysis (8). All of the cases had malignancy. In addition, 7 cases were related to haematological malignancy. In 7 cases, the malignancy could not be surgically removed. Four cases were treated with PE; however, not all patients survived (8). Auto-antibodies were evaluated several times during the course in only 2 cases, including the current case (7). Although PE is assumed to be effective for TEN patients due to the removal of inflammatory cytokines, it appears to be difficult to treat TEN/SJS-like PNP with PE. To treat PNP patients with PE without treating their cancers would be equivalent to treating TEN patients with PE without discontinuing causative drugs. It is desirable to detect and treat cancers before eruptions spread to the whole body. Considering the tolerability of cancer patients for invasive treatments, it is important to make careful decisions about treating TEN/SJS-like PNP patients with PE.
It has only been reported in mouse studies that PNP is associated not only with humoral, but also with cell-mediated, autoimmune reactions (1). Although there are some reports of PNP in which either immunoblot analysis or immunohistochemical analysis were performed (7, 10), there are no reports of human TEN/SJS-like PNP in which both immunoblot analysis and immunohistochemical staining were performed before and after PE. Transitions of both immunoblot analysis and immunohistochemical staining were important in order to evaluate how PE affects patients with PNP, because PNP is associated with both humoral and cell-mediated autoimmune reactions (1). We hypothesize that cell-mediated immunity plays a major role in the pathogenesis of TEN/SJS-like PNP, as skin erosions spread, despite reduction in cytokines and autoantibodies with repeated PE in the current case and another case report (5). In the current case, immunohistochemical staining revealed that more CD8+ cells had infiltrated into the epidermis than CD4+ cells in the first biopsy specimen (Fig. 1h, 1i). Some reports of PNP show that more CD4+ cells infiltrated into the epidermis than CD8+ cells (10). CD4+ and CD8+ cells produce interferon-γ, and CD8+ cells secrete cytotoxic molecules (11). It is possible that the predominance of CD8+ cells might mean a predominance of cell-mediated immunity. In this case, CD8+ cells in the epidermis did not decrease after PE (Fig. 1j), which could explain the insufficiency of PE for TEN/SJS-like PNP. It is difficult to confirm this result in many cases, and further investigations, such as using tissue from biobanks, are required.
We consider that some TEN patients might be diagnosed with PNP if more investigations were carried out. In case of SJS/TEN-like patients without specific medication history, the possibility of PNP should be considered, and systemic evaluation for haematological malignancy, ELISA tests and IB analysis performed.


 Click to show fullsize
Click to show fullsize